An Uncommon Presentation of Breast Adenomyoepithelioma: A Case Report
Abdullah Mohammed Alshamrani*, Abdullah Ahmed Alzarea, Muruf Zaid Alshalwah, Eman Ali Alrabee, Alrasheedi Saud D
General Surgery Department, Security Forces Hospital Program, Riyadh, Saudi Arabia
*Corresponding author: Abdullah Mohammed Alshamrani, General Surgery Department, Security Forces Hospital Program
P.O. Box 3643, Riyadh 11481 Saudi Arabia. Tel: 0096655 326 6990; Email: alshamraniabdullah92@gmail.com
Citation: Alshamrani AM, Alzarea AA, Alshalwah MZ, Alrabee EA, A D Saud (2020) An Uncommon Presentation of Breast Adenomyoepithelioma: A Case Report. Annal Cas Rep Rev: ACRR-103.
Received Date: 06 March, 2020; Accepted Date: 11 March, 2020; Published Date: 17 March, 2020.
Abstract
Background: A breast adenomyoepithelioma is an uncommon tumor characterized by the presence of epithelial and myoepithelial cells. Case Report: We describe a 47-year-old woman who presented with a right breast mass of four-year duration. An examination of the breasts revealed two masses in the right inner quadrant of the right breast measuring 1 x 1 cm and 2 x 2 cm in dimension. A mammogram favored a lesion highly suspicious of malignancy, suggesting further examination. An ultrasound examination confirmed the mammography and a biopsy was subsequently performed. A biopsy revealed findings suggestive of duct adenoma. The tumor was excised, and the specimen was sent for histopathological examination. The histopathological findings were consistent with adenomyoepithelioma. The patient was discharged one day after surgery and did not present any complaints.
Conclusion: Although most adenomyoepitheliomas have a benign course, it is essential for clinicians to identify these tumors, as the radiologic and cytologic characteristics can mimic malignant lesions. A definitive diagnosis can be made after a histopathologic examination, and tumor excision may be helpful in preventing recurrence or malignant change.
Keywords: Adenomyoepithelioma, breast, myoepithelial cells, neoplasm
Introduction
Breast adenomyoepitheliomas are rare tumors characterized by a biphasic neoplastic proliferation of luminal and myoepithelial cells around small epithelial lined spaces [1]. These tumors have been described to have several histologic patterns, including the tubular, lobulated, or spindle subtypes [2]. The spindle subtype is primarily composed of spindled myoepithelial cells with visible epithelial lined spaces that may be challenging to identify in some sections. Consequently, this subtype may be erroneously mistaken for a leiomyoma [2]. The tubular growth pattern is composed of small, round tubules lined by luminal epithelial cells. Although this subtype has a histologic pattern similar to that in tubular adenomas, it is characterized by more prominent and hyperplastic myoepithelial cells. The lobular subtype comprises clear, eosinophilic, or plasmacytoid myoepithelial cells proliferating around epithelial-lined spaces [2].
Many adenomyoepitheliomas are benign and the standard treatment is tumor resection with negative margins [3]. However, there have been cases of local recurrence or isolated metastasis to the lymph nodes, and some cases of malignant transformation have been reported [4]. Given that these tumors are rare, few reports have described the clinical presentation and histologic findings in patients with breast adenomyoepitheliomas [3,5]. We report a case of an uncommon presentation of breast adenomyoepithelioma in a middle-aged woman.
Case Report
A 47-year-old woman presented with a complaint of a right breast mass of four-year duration. Her history was remarkable for hypertension and dyslipidemia. She also reported experiencing trauma to the right breast after an object fell on it, which caused bruising to the breast; however, she ignored it.
One year later, the patient noticed a right breast mass, which was painless and did not change in size. However, she did not seek medical advice. Two years later, she was offered a mammography during a breast awareness campaign and was subsequently transferred to our hospital for further evaluation of the breast mass.
The patient had no history of nipple discharge, skin changes, or masses in other parts of the body. Her menstrual cycle was regular, and she was nulliparous. No family history of breast cancer was reported.
An examination of the breasts revealed two masses in the right inner quadrant of the right breast measuring 1 x 1 cm and 2 x 2 cm in dimension. The masses had irregular borders and were fixed. There was no nipple discharge or retraction. There were also no skin changes or palpable axillary lymph nodes. The left breast was normal with no palpable axillary lymph node.
A mammogram showed a round, dense lesion measuring 3.5 x 3.8 cm in the right breast and another measuring about 1 cm in dimension (Figure 1).
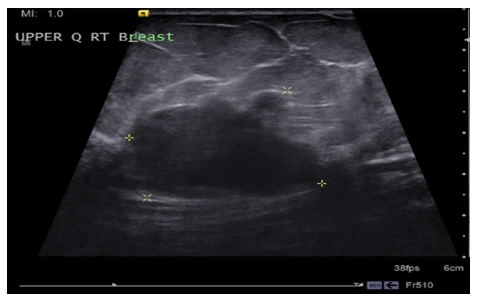
Figure 1: Mammography of the right breast showing a dense, rounded, posteriorly-lesion with fairly well-defined lobulated margins measuring 3.5 x 3.8 cm. Also observed is a smaller, anteriorly-located lesion measuring approximately 1 cm. No cluster of microcalcification is seen.
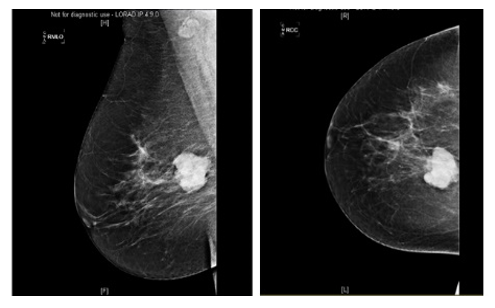
Figure 2: Ultrasound showing a posteriorly-located hypodense lesion with irregular lobulated margins measuring approximately 3.6 x 3.6 cm in the upper quadrant of the right breast. A smaller, adjacent lesion measuring 1.2 x 0.6 cm is also noted.
CT scan done, the study revealed right breast lobulated enhanced soft tissue mass lesion that measure about 3.8 x 3.2 cm consistent with presumed right breast cancer. Also noted is adjacent small nodular lesion. Benign looking bilateral axillary lymph nodes are seen (Figure 3).
There was no cluster of microcalcification. The right breast was classified as breast imaging reporting and data system (BI-RADS) 5, and the left one was classified as BI-RADS 1. Axillary lymph nodes were observed in both axillae. An ultrasound of the breasts showed a hypodense lesion with irregular margins in the upper right breast measuring 3.6 x 3.6 cm and another lesion measuring 1.2 x 0.6 cm (Figure 2). The left breast was normal. No axillary lymph nodes were observed. However, the lesion described in right breast was suspicious for malignancy, and a biopsy was recommended.

Figure 3: The study revealed right breast lobulated enhanced soft tissue mass lesion that measure about 3.8 x 3.2 cm consistent with presumed right breast cancer. Also noted is adjacent small nodular lesion. Benign looking bilateral axillary lymph nodes are seen.
Biopsies were obtained from her right and left breasts for histopathological analysis. An examination of the specimen obtained from the right breast showed a benign proliferative lesion suggestive of duct adenoma. A histopathological examination of the left breast tissue showed ductal epithelial hyperplasia, and the specimen was negative for malignancy.
Wide local excision and frozen section under general anesthesia were offered. A circumferential skin incision was made, and the wide local excision extended in the right upper inner quadrant deep into the pectoralis fascia. The specimen was marked and sent for frozen section; the result was consistent with a benign lesion. The skin was closed using staplers. No drain was inserted. The patient was extubated and transferred to the recovery room in good condition. She was subsequently transferred to the ward.
Her postoperative was unremarkable, and she was discharged one day later. Histopathology of the specimen was consistent with adenomyoepithelioma. The tumor measured 3 x 3 x 2 cm in size, with involvement of the lateral and deep margins. Other peripheral margins were free of adenoepithelioma, and fibroadenoma was noted within the specimen measuring 1 cm.
Discussion
Breast adenomyoepitheliomas are unusual tumors commonly reported in middle aged women [3]. These tumors present as single, well-circumscribed rounded nodules of varying sizes (0.5–5 cm), with a median size of 1.5 cm [6]. They are typically firm but may be soft in consistency or have poorly defined margins. These tumors can be located either peripherally or centrally near the areola and can be felt as a rounded nodule during physical examination [7]. Typical histological features of these tumors include myoepithelial cells, which can appear as small, ovoid, dark nuclei, localized either above or below the plane of focus of the ductal epithelium, or dispersed in the cellular environment as bipolar, bare nuclei [2]. The myoepithelial cells display different histologic patterns but hardly show atypia [6].
In some cases of breast adenomyoepithelioma, cancer can arise in the epithelial or myoepithelial component, or both [2]. In the present case, no histologic evidence of malignancy was found. As was the case in our patient, most patients with breast adenomyoepitheliomas do not have a history of malignancy or concomitant malignancy. In one series including 14 patients with breast adenomyoepitheliomas, 11 cases had no prior or concomitant malignancy [3]. However, these tumors have the potential to become malignant [4], with some cases reported to harbor synchronous epithelial malignancies [2].
A biopsy was recommended in our case because a mammography exam showed signs suggestive of malignancy. Although a core biopsy showed a benign proliferative lesion suggestive of duct adenoma, it should be underscored that this procedure should be challenged as a diagnostic tool in breast neoplasms—clinicians in some countries are no longer advised to request this procedure due to the absence of proper training facilities [7]. A wide excision was subsequently performed in our patient, and a histopathologic examination showed findings consistent with adenomyoepithelioma. A fibroadenoma was also noted within the specimen. Of note, a fibroadenoma may be confused with the tubular subtype of an adenomyoepithelioma. In contrast to fibroadenomas, which are composed of staghorn epithelial cells and fibrillary stroma, adenomyoepitheliomas exhibit a dense stroma, with epithelial and myoepithelial cells arranged in a typical tubular pattern [8]. Further investigations, such as immunohistochemical staining, may show a biphasic cellular pattern with proliferative myoepithelial cells, which is a critical component in diagnosing adenomyoepitheliomas [7].
Unfortunately, immunohistochemical staining was not requested in our patient because the pathologist determined that the biopsy findings were consistent with a duct adenoma.
In our case, a mammogram showed a round, dense lesion in the right breast with no sign of microcalcification, and this was classified as BI-RADS 5. In a previous report, it was found that all the cases of breast adenomyoepithelioma showed BI-RADS classifications of ≥ 4, which should prompt a clinician to request a biopsy [3]. Although there’s no report of the proportion of patients with breast adenomyoepithelioma who have a BI-RADS classification < 4, some investigators found that only 2 of 310 patients with ultrasonographic features in favor benign disease were later diagnosed as adenomyoepithelioma [9]. Our non-finding of microcalcifications in this patient is in line with reports of imaging studies that showed that calcifications were rare in breast adenomyoepitheliomas [3,10]. An ultrasound examination in our report showed the typical findings of adenomyoepitheliomas that include a small, irregular, well-to-poorly circumscribed hypodense mass [3].
While most adenomyoepitheliomas have a benign course, some authors have reported that a mastectomy was offered to a small proportion of these patients [3]. In some cases, an excisional biopsy was offered, and the outcomes were reportedly favorable, as was the case in our patient, who was offered a wide excision biopsy. According to one report, a wide excision with negative margins may be a rational approach in patients with adenomyoepithelioma, and it may offer a long-term solution to avoid local recurrences and decrease the risk of malignant change [7].
Conclusion
Overall, breast adenomyoepitheliomas are rare tumors comprised of epithelial and myoepithelial cells. Although most adenomyoepitheliomas have a benign course, it is it is essential for clinicians to identify these tumors, as the radiologic and cytologic characteristics can mimic malignant lesions. A definitive diagnosis can be made after a histopathologic examination, and tumor excision may be helpful in preventing recurrence or malignant change.
References
- Lakhani S, Ellis I, Schnitt S, Tan P, van de Vijver M. WHO Classification of Tumours of the Breast [Internet]. [cited 2019 Aug 9]. Available from: https://publications.iarc.fr/Book-And-Report-Series/Who-Iarc-Classification-Of-Tumours/WHO-Classification-Of-Tumours-Of-The-Breast-2012
- Tavassoli FA (1991) Myoepithelial Lesions of the Breast. Myoepitheliosis, Adenomyoepithelioma, and Myoepithelial Carcinoma. Am J Surg Pathol 15: 554-568.
- Moritz AW, Wiedenhoefer JF, Profit AP, Jagirdar J (2016) Breast Adenomyoepithelioma and Adenomyoepithelioma with Carcinoma (malignant Adenomyoepithelioma) with Associated Breast Malignancies: A Case Series Emphasizing Histologic, Radiologic, and Clinical Correlation. Breast 29: 132-139.
- Yoon JY, Chitale D (2013) Adenomyoepithelioma of the Breast: A Brief Diagnostic Review. Arch Pathol Lab Med 137: 725-729.
- Bhatkule. Clinical Cancer Investigation Journal [Internet]. [cited 2019 Aug 9]. Available from: http://www.ccij-online.org/article.asp?issn=2278-0513;year%3D2013;volume%3D2;issue%3D1;spage%3D57;epage%3D59;aulast%3DBhatkule#ref2
- Harigopal M, Park K, Chen X, Rosen PP (2004) Pathologic Quiz Case: A Rapidly Increasing Breast Mass in a Postmenopausal Woman. Malignant Adenomyoepithelioma. Arch Pathol Lab Med 128: 235-236.
- Catena F, Santini D, Di Saverio S, Ansaloni L, Taffurelli M (2008) Adenomyoepithelioma of the Breast: An Intricate Diagnostic Problem. Breast Care (Basel) 3: 125-127.
- Cangiarella J, Simsir A. Orell and Sterrett’s Fine Needle Aspiration Cytology [Internet]. 5th ed. Elsevier; 2012 [cited 2019 Sep 2]. Available from: https://linkinghub.elsevier.com/retrieve/pii/C20090495321
- Park Y-M, Kim E-K, Lee J-H, Ryu J-H, Han S-S, et al. (2008) Palpable breast masses with probably benign morphology at sonography: can biopsy be deferred? Acta Radiol 49: 1104-1111.
- Adejolu M, Wu Y, Santiago L, Yang WT (2011) Adenomyoepithelial Tumors of the Breast: Imaging Findings With Histopathologic Correlation. American Journal of Roentgenology 197: W184-W90.